
Do you have a loved one with Down syndrome?
Have you ever wondered how much they are worth?
$74,768.91
Give or take a bit in kiwi dollars – that’s 38,000 British Pounds at today’s exchange rate.
That’s according to this report for the New Zealand National Screening Unit (NSU) that was prepared by Health Outcomes International (HOI). The NSU engaged HOI in 2007 to:
“…inform its decision as to whether a national antenatal screening programme for Down syndrome should be established in New Zealand.”
That programme was implemented in 2010.
The report is quite long, running to 68 pages. It mostly covers technical aspects of screening and the practicalities of delivering a national screening programme.
It also talks about the costs effectiveness of running a national screening programme for Down syndrome.
Warning: It’s not nice.
“A further assumption regarding the establishment of formal screening programmes is that the programme will be cost beneficial for the population, and the health system.”
and
“….the economic costs of screening outweigh the high costs associated with the long term care needs of an individual with Down syndrome.”

“It is cost effective as the estimated cost of avoiding the birth of a baby with Down syndrome (about 38,000 pounds) is substantially less that the lifetime costs of care.”
“while some may feel that the cost of about 40,000 pounds sterling to prevent the birth of a baby with Down syndrome to a woman under 30 may be expensive, it is low compared with the costs of caring for someone with Down syndrome.”


Which is uncomfortably close to this:
“60,000 Reichsmark is what this person suffering from a hereditary defect costs the People’s community during his lifetime. Fellow citizen, that is your money too.”
That is from the Action T4 euthanasia programme. Eugenics. See how they both talk about the costs (read “burden”) of care as a justification for not having them amongst us.
The report also talks about the benefits of screening. They actually mean effectiveness:
“Down syndrome screening programmes are effective in detecting Down syndrome abnormality.”

In the section on “benefits of screening” there is no identification of any therapeutic benefit to the one with Down syndrome, or the mother.
“Reproductive decisions” are listed as a benefit:
![]()
Termination is mentioned 17 times in the report.
Bottom line. If you have a child with Down syndrome, they reckon they’re worth $74,768.91, more or less. That’s how much of our money they are happy to spend to stop our children being born.
That’s not nice.
It’s not just the NSU in New Zealand. Most of the research links back to the United Kingdom. THE UK National Health Service have “The Decision Planning Tool (DPT)” This is:
“… an instrument to aid Trusts, commissioners and health professionals plan, improve and monitor Down’s syndrome screening practices by assessing the costs and effects of first and second trimester screening strategies.”
There’s that word cost again. But this time, the costs and effects are measured by a thing called TOP: Termination of pregnancy, on sheet 8 of their spreadsheet:
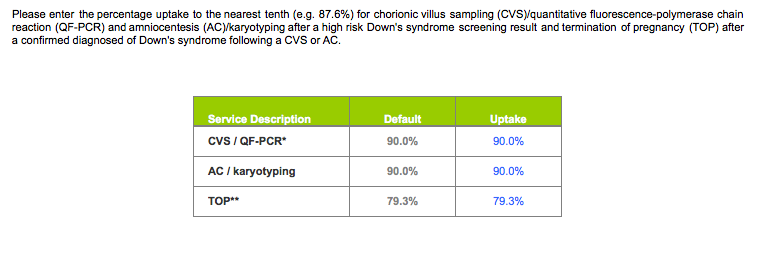
Bottom line. A termination rate of 79%, more or less, makes an effective national screening programme.
That’s not nice.
We like to be nice. Our position statement on screening says:
“We acknowledge that for some, antenatal screening and diagnostic testing may reassure parents or help some parents prepare for the birth of a child with Down syndrome. We believe that any antenatal screening and diagnostic testing must respect the life and integrity of the unborn child, cause no harm, be only directed towards safeguarding or healing the unborn child and be presented in a way that does not discriminate against people with Down syndrome.”
It looks like others may have a different agenda.
It would seem to be more about money and termination rates.
Or eugenics.
We would prefer unconditional love, acceptance and respecting basic human dignity.
]]>{kind=link}
Important win secured with revised screening guidelines
Saving Downs has secured a number of important and welcome changes to the national screening programme for Down syndrome.
Last week new guidelines were formally issued by the National Screening Unit. These were revised following the upholding of our complaint to the Health and Disability Commissioner in 2010.
Saving Downs considers that the new documents are a significant improvement and an important win in the journey towards realising social justice for the Down syndrome community.
Spokesman Mike Sullivan explained that “The overarching change in these documents is a new emphasis towards the help and guidance available for mothers and their pregnancies throughout the screening pathway. There is a noticeable shift away from the offensive prominence of the disability selective termination option in the original documents.”
One of the most welcome changes is the policy move away from the routine offering of screening to all pregnant women to simply advising them of the availability of screening. “That’s an important distinction as the onus is now on parents to request participation as a choice, rather than it being a matter of routine pregnancy care” Mr Sullivan explained.
Mr Sullivan also observed that although the new documents are welcome, Saving Downs remains committed to ensuring that antenatal screening is limited to providing life affirming care. New Zealand law currently provides a lesser degree of protection of life before birth based on disability, which is discrimination. Saving Downs will continue to work to repeal this law, a process that is now underway in the UK with a Parliamentary inquiry into abortion on the grounds of disability. Saving Downs have accepted an invitation to participate in that inquiry.
Mr Sullivan hopes that with the new guidelines, more pregnant women who are faced with an unexpected diagnosis will receive the loving and life affirming support to continue their pregnancy that they deserve.
Further reaction to the new guidelines is discussed in this blog.
]]>Last week new guidelines for screening for Down syndrome in New Zealand were formally issued by the National Screening Unit. These consist of a leaflet for pregnant women and their partners and detailed guidelines for Health Practitioners. These have both been revised following the upholding of our complaint to the Health and Disability Commissioner in 2010. The Commissioner ruled that the previous documents could be “more comprehensive and accessible”. We also made detailed submissions on the drafts of these new documents last April.
The new documents are a significant improvement on their predecessors and an important victory in our ongoing advocacy for the full recognition of human rights for our community.
The overarching change in these documents is a new emphasis towards the help and guidance available for mothers and their pregnancies throughout the screening (and diagnostic testing) pathway. There is a noticeable shift away from the offensive prominence of the disability selective “termination option” in the original documents. The new documents are probably the best we can expect in the light of the New Zealand abortion law allowing discrimination against those with a disability – more on that later.
It is these types of small, patient steps that will win this race. So, the new focus on help and guidance and respect for the Down syndrome community is most welcome, as one of these steps in our journey for social justice.

Now, let’s look at some of the specific changes that we have secured.
The most significant change is the policy move away from the routine offering of screening for Down syndrome to all pregnant women to simply advising them of the availability of screening. This was announced in our press release in May last year. Well respected and prominent New Zealand journalist Kerre Woodham had this to say about the shift in focus in her great editorial in the New Zealand Herald in June 2012:
“It’s a subtle shift in emphasis but an important one because a growing number of people, health professionals included, believe that Down syndrome in itself is not a good enough reason to terminate a pregnancy.
And I would concur. It’s a personal choice and not everyone is going to think the same way, but having worked with a number of children and adults with Down syndrome, having enjoyed the humour and the wit and the work ethic of a number of young men and women with the condition, I can’t see how anyone would consider a person born with Down syndrome to have any less right to be on the planet than those born free of it.”
Kerre concluded her editorial with:
“If you think that by terminating the pregnancy, you’d be doing the child a favour, I recommend you ask a person with Down syndrome what they would choose.”
And that pretty much says it all really – thanks Kerre!
By changing the requirement from “offering” screening to simply “advising” pregnant women of its availability, the onus is now on parents to request participation as a choice, rather than it being a matter of routine pregnancy care. That’s an important distinction.

Turning to the new pregnancy leaflet, there are a number of important changes that are all a direct result of our advocacy.
Importantly, it is made very clear that screening is optional and a matter of choice, rather than routine. It is clearly laid out that it is optional to enter the screening pathway and optional to leave it at any point. Those choices must be respected.
The leaflet now includes pictures of a pregnant woman along with her partner. The previous versions were text only. So, we are seeing the human dimension.
There is now a picture of a family with their children, including a cute one with the extra love chromosome; acknowledging in a positive way the human face of Down syndrome.
There is now an ultrasound image of an unborn child, so we are clear on the other human life that is involved in this process.
There is now a diagram showing how a diagnostic test is done with a needle inserted into the placenta, next to the unborn child – that will ring alarm bells for some and reinforces the risk to the other life involved.
It is now made clear that all conditions cannot be determined through screening. That’s an important distinction.
It is now acknowledged that Down syndrome is present from conception, recognising that the condition is a part of the naturally occurring range of human life that starts at conception.
Down syndrome is now largely presented in a more positive light. The focus on health problems is disappointing though, as all people experience a range of health issues as part of the human condition. The previous versions were certainly very disrespectful towards those with Down syndrome.
The difference between screening and diagnostic testing is now properly explained, which will hopefully address widespread confusion around this.
Results are now referred to as “chance” rather than the negative “risk” we have long wanted to wave goodbye to. Our children are not risks, so we wave that one goodbye!
The risk of diagnostic testing was under presented in previous versions. Now it is properly detailed:
“For every 200 women who have a diagnostic test, one or two will have a miscarriage as a result of the test.”
The guidelines explain further that for every 1000 women screened, about 50 will receive an increased chance result and two will be diagnosed with a baby with Down syndrome or another condition. A screening cut-off of 1:300 is used to detect 85% of babies with Down syndrome. There is no discussion, however, as to why it is necessary to detect these babies.
If you do the maths, for every 200 women who have a diagnostic test, there will be one or two miscarriages from the test to find eight unborn children with Down syndrome or another condition. In other words, it’s a dangerous business. In fact, there is no life affirming intervention that relies on a positive diagnosis of Down syndrome where the statistical (average) benefit is greater than the chance of death from the diagnostic test. This means that the screening pathway is non-therapeutic as defined by medical practice. On this, we included in our submission on the draft guidelines a request that:
“Pregnant women and their partners must be advised that participation in the screening pathway imposes more harm than benefit to their unborn child, through miscarriage and morbidity due to diagnostic testing”.
But you won’t see that implicitly stated in the guidelines. However, it can be established by examining the data on risks of diagnostic testing. We have discussed this issue before in our blog Screening for Down syndrome: is it therapeutic?

The new guidelines for health practitioners support practitioners advising about the availability of antenatal screening for Down syndrome. There is a raft of important changes to these guidelines with over 85% of the issues we submitted on being resolved. A number of these are somewhat medically technical in their nature, so I won’t be getting into the detail of those. Suffice to say that these have been resolved and it seems surprising that our own specialist had to point out basic errors in the NSU’s draft guidelines. We can just be happy that they have been sorted out and the guidelines are now more closely aligned with the principle of providing detailed, factual and evidence based information; this was poorly lacking in the previous versions.
The earlier guidelines had incorrect information on the risk of miscarriages and no details about complications caused by diagnostic tests. These have now been corrected:
“The risk of miscarriage after amniocentesis is about one miscarriage in every 100–200 women tested.”
“The risk of miscarriage after CVS is about one miscarriage in every 50–100 women tested.”
“Other rare complications include leaking of amniotic fluid and infection of the uterus or foetus.”
As discussed above these are significant hazards to find a very low number of unborn children with Down syndrome. Parents deserve to know that.
For the first time there is acknowledgement of the potential mental harm associated with screening and diagnostic tests:
“The potential harms …. include anxiety and stress associated with the screening process”.
Maternal anxiety and foetal hazard in the screening and testing process are known accompaniments. The former can disrupt bonding between mother and child with added psychosocial ramifications of pregnancy loss, while the loss of a child through a non-therapeutic investigation is usually considered a tragedy. It was remiss of the NSU not to advise parents of this risk earlier, it has been well documented since 2006.
There is now clarification that the 18 to 20 week anatomy scan is another screening test for conditions such as Spina Bifida and can present markers for other conditions. This has always been an area of confusion, with many parents using this ultrasound scan for a social “look at their child” and not realising the implications that this is in fact a screening test for the pregnancy. Parents need to understand these things. It is not good enough to go in for a “social scan” and come away with something you are not prepared for.
The section on communicating positive diagnostic results has been much improved with more information and support available for continuing the pregnancy. It is implicitly stated that health practitioners must support a women continuing with a pregnancy. Hopefully that will address the type of problem we experience in New Zealand where women are encouraged to have late-term abortions for Down syndrome and Spina Bifida. Now that there are clear guidelines against this practice we will be able to hold health practitioners accountable for their actions. Encouraging abortion has to stop. It lowers the dignity of the child, the parents and those living with disability. We will be keeping a very close eye on things in this regard.
It is good to see postnatal palliative care presented as an option where a baby is expected to have a very short life expectancy. This has never been included as an option previously and provides for a natural process of passing and healing. It will also help towards mitigating situations where parents have been given little hope for their children, and those children go on to have great lives.
The NSU have done a reversal in the area of monitoring. Previously they refused to monitor the effect of the screening programme on the birth prevalence of Down syndrome. Following our submission, there is now a specific requirement to monitor the outcomes of pregnancies in the screening pathway. This is something we will be watching very closely.

So, that’s it in a nutshell for the new leaflet and guidelines. They are probably the best we can expect in the light of the New Zealand abortion law allowing discrimination against those with a disability.
Laws that make provision for abortion on the basis of a disability afford less legal protection to one section of our society than another, solely based on ability and biological difference. These laws are based on a view that the life of a person with a disability is of less worth, warranting a lesser level of legal protection. The law has been set up expressly to avoid the birth of people with disabilities. This is both discrimination and eugenics. It devalues the lives of all people living with a disability by establishing in law that those with a disability have fewer rights than others.
We will continue working on the repeal of foetal abnormality as grounds for abortion in New Zealand. This process is now underway in the UK with a Parliamentary inquiry into abortion on the grounds of disability. We have accepted an invitation to make a submission to that inquiry. Any positive change in law and policy from that inquiry will inevitably have downstream benefits in New Zealand and other countries that have discriminatory disability selective screening programmes.
In closing, let us remember that pregnant women enter into trusted relationships with health care providers to receive nurturing of their unborn child. When faced with an unexpected diagnosis, the dignity of their child hasn’t changed and that woman deserves loving and life affirming support to continue with her pregnancy. Offering an abortion is not a civilised, loving, or compassionate response to a disabling condition. It lowers the dignity of the unborn child, the parents and the disability community. The new emphasis towards the help and guidance available for mothers and their pregnancies throughout the screening pathway is an important step in the journey to realising social justice for our community.
]]>In reflecting on what we have achieved, I am reminded of the reality that all great social justice causes take a long time to evolve, and success comes through many small steps. It took William Wilberforce a lifetime to abolish the slave trade, but abolish it, he did. His example is an inspiration for us. In his own words:
“You may choose to look the other way but you can never say again that you did not know.”
So a key area of our work has always been to raise awareness of the discriminatory and eugenic practice of antenatal genetic screening and disability selective abortion in New Zealand. Our work has had widespread media coverage in newspapers and mainstream TV news throughout 2012. People may choose to look the other way but they can no longer say that they do not know what is going on.

Another famous quote of William Wilberforce is:
“We are too young to realize that certain things are impossible… So we will do them anyway.”
And that is what we are doing. People said we wouldn’t turn this around, but we said – we will do it anyway, because we can. Our families deserve nothing less of us.
So let’s reflect on all those great results we have achieved over the last year and celebrate how far we have come. To put this in context, it looks as though we may well have stemmed what was a decreasing number of births of babies with Down syndrome in New Zealand as a result of screening and selective abortion. In fact we may have even turned the tide on this. From 2007 to 2010, there was an average of 52 births per year of babies with Down syndrome. In 2011 there were 60, the first full year after the infamous “quality improvements” that were introduced in March 2010. Its early days, and we must be vigilant, but this is promising and going in the right direction.
The scene was actually set back in October 2011, when Diane Belcher from Spina Bifida NZ and I met with David Rutherford, the Chief Commissioner of the Human Rights Commission (HRC) to discuss our concerns relating to the practice of antenatal screening for Down syndrome and other conditions. David kindly indicated a willingness to formally receive our expert opinion from a world expert on the Convention on the Rights of Persons with Disabilities (CRPD) in terms of that conventions application in the area of antenatal screening for disability. A formal submission was made in April 2012 and was supported by these seven disability advocacy organisations:
- Down Syndrome International,
- The New Zealand Down Syndrome Association,
- Disabled Persons Assembly NZ Inc,
- People First New Zealand Inc. – Nga Tangata Tuatahi,
- The Tiaho Trust,
- Spina Bifida Association of New Zealand, and
- Savingdowns.
That submission asked the HRC to generally enquire into the New Zealand screening programme, develope an action plan where there are areas of conflict between the programme and the CRPD, and oversee and monitor the implementation of such an action plan. The submission has now been considered and we are expecting a formal response over the next few days. This has the potential to have many positive benefits. That seven disability advocacy organisations are supporting this initiative gives it much strength and credibility. I am confident that this will do well for our cause.
Also in April the New Zealand Down Syndrome Association (NZDSA) adopted a revised position statement on screening. This followed a membership review that was advocated by Saving Downs. The new position statement includes this:
“The NZDSA advocates that the primary goal of prenatal screening should not be to reduce the birth prevalence of Down syndrome in the population, but rather to improve prenatal health care and delivery care for the mother and baby”.
This was a significant shift away from what was previously a somewhat “sitting on the fence” position.
For the first time the NZDSA also adopted this position statement on terminations:
“The NZDSA does not consider Down syndrome in itself a reason for a termination”.
These are powerful advocacy statements that put a firm line in the sand and recognise that true advocacy is about people with Down syndrome. They are closely aligned to our own mission statement:
“To ensure that antenatal screening exists only to provide unborn children with Down syndrome and their parents with life-affirming, unbiased care through education, support and understanding.”
What we have witnessed here is a quantum, and most welcome, shift in advocacy from the NZDSA on this issue. That is a reflection on the lift in awareness in our community and the wider public on the discriminatory and eugenic nature of screening in our country. That is the strength in raising awareness around the issue. It was that same awareness that brought the seven disability advocacy organisations together for the CRPD submission to the HRC.
Also in April (man that was a busy month) Saving Downs made detailed submissions on the National Screening Unit’s (NSU) draft revised information pamphlets and guidelines for health practitioners in relation to the screening programme for Down syndrome. These documents are being revised because in 2010 a complaint from Saving Downs was upheld by the Health and Disability Commissioner on the unbalanced quality of information produced by the NSU.
Two key areas of our submissions are that pregnant women and their partners must be advised that:
- Participation in the screening pathway imposes more harm than benefit to their unborn child, through miscarriage and morbidity due to diagnostic testing, and
- That any benefit to the unborn child should be investigated as late as feasible in the pregnancy, to avoid harm.
We have also submitted that the NSU consumer pamphlet and guidelines be amended to recognise that an abortion on the basis of a diagnosis of an unborn child with Down syndrome is unlawful, as it does not meet the test of “a serious handicap” required under New Zealand law.
As part of the submission process the NSU has already agreed to move away from the routine offering of screening for Down syndrome to all pregnant women to simply advising them of the availability of screening. By changing the requirement for midwives and GPs from “offering” screening to simply “advising” pregnant women of its availability, the onus is on the parents to request participation, rather than it being a matter of routine pregnancy care. Midwives and GPs who are morally opposed to eugenics can exercise their right to conscientious objection and advise parents to seek the “service” elsewhere with no requirement to provide a referral.
This is a significant win for us.
Let me say that again. This is a significant win for us.
This is why it is a significant win for us. When the NSU ran training workshops on screening for Down syndrome in May this year, feedback from midwives and GPs indicated a growing opposition to the screening programme, on the grounds that the eugenic undertone is unethical. Doctors and midwives were challenging the NSU in the workshops, outlining concerns that the screening programme was unethical and devalued a vulnerable section of our community. Again we see a lift in awareness on the discriminatory and eugenic nature of screening in our country, by the very professionals at the coal face. It is very encouraging to know that we have these professionals not only sharing our concerns, but also speaking out and refusing to participate in the programme. Reports like this editorial in the Sunday Herald show how this change is recognised in the wider community as an important development in recognising the inherent dignity and worth of people with Down syndrome.

The training workshops didn’t actually go too well for the NSU this winter. The Nelson and Wellington sessions had GPs and midwives opposing the programme. The Whangarei workshop was cancelled after I turned up and asked to sit in on the session (I was invited to attend by our local midwives group). Attendees at New Plymouth had to walk pass the adults with Down syndrome handing out our factsheet about screening. In Tauranga, supporters who happened to have Down syndrome laid out our leaflets on the chairs whist the participants came in to learn about how to screen them out. Oh dear. That’s what happens when the NSU excludes us from such things.
Bizarrely, the training workshops were held in April, May and June whist the NSU was still reviewing the submissions on the proposed new guidelines. Even the New Zealand College of Midwives, who were contracted to run the training sessions, were left confused, saying this in their submission to the NSU:
“we are a little perplexed regarding the timing of the revisions of these resources”
They were perplexed because they were running training sessions on the draft revised guidelines for the NSU whilst the submissions on those guidelines were still being considered by the NSU. The NSU has advised that the new guidelines and pamphlets have now been completed and will be issued in December, some 6 months after the training sessions. We will blog those when they come out.
April was a good month for Saving Downs. The NSU training workshops were good for Saving Downs too.

In July I headed across the ditch to Melbourne to present our work to Right to Life Australia. As a group we do not get involved in the mainstream pro life/pro choice stuff. We focus on screening and the related issues of discrimination and eugenics, with abortion being recognised as the means of eugenics against our community. Where an organisation opposes eugenics and supports our mission statement, we are open to sharing our message. Right to Life Australia oppose eugenics, so I went to share the word. Our work was well received and the seeds planted for our work to be taken forwarded into Australia, where it is certainly needed.

Also in July the Prosecutor of the International Criminal Court (ICC) decided to initiate a formal preliminary examination into a complaint laid by Saving Downs against the New Zealand Government’s antenatal screening programme for Down syndrome and other conditions. This was an outstanding achievement in its own right as it indicated that the ICC was taking the complaint very seriously and that the case has sufficient merit to warrant comprehensive legal analysis.
In November the prosecutor indicated that additional facts and information are required to enable the ICC to have jurisdiction to proceed with further analysis. We are currently awaiting the new NSU guidelines and the outcome of the CRPD submission to the HRC before proceeding on the submission of further information in support of our case.
The complaint before the ICC has had widespread media coverage globally and is a powerful strategy to raise awareness around this important cause for social justice. I spoke about it on breakfast news on TV one.

In August we had our awesome seminar “Loving Every Child: Defying Eugenics”. Here is how one attendee described it:
“The whole seminar took me on a roller coaster ride of emotions that varied as wide and far as the speakers presenting, inspiration, joy, compassion, outrage, horror, disbelief, anger, admiration all churned together in a sometimes gut wrenching knot as I was enlighten of the full picture, the whole truth of this insidious screening process for Down Syndrome and Spina Bifida in New Zealand.”
See our blogs about the seminar:
Loving every child – a mothers perspective
Down syndrome screening – seeing eugenics through the fog
Down syndrome screening – we must draw the line here now
The seminar coincided with the launch of our new web site. This has been a great success and we are approaching 10,000 hits. Social media is where it’s at for social justice causes such as ours. Our blog about Professor Stone, his role as an adviser to the NSU and his involvement in pregnancies involving Down syndrome attracted over 1,700 hits alone. That blog has been removed after threats of libel action, which we are not resourced to defend. It would have provided a great avenue for raising more awareness around this issue. It’s sort of funny though, we know what’s going on, they know what’s going on, and they know that we know, but we still get smoke and mirrors. This blog outlines how mothers are being encouraged to have late term abortions for Down syndrome in New Zealand. This is the real stuff folks, and why we have to keep up our important work.

In October I was privileged to visit Europe to support the Stop Eugenics Now initiative. This was a great opportunity to share our work and pass it forward. They are very organised and passionate about defending our community against eugenics in Europe and I look forward to seeing how their work unfolds.
So, that is where things sit after a year of successful advocacy in New Zealand.
The time is right now for other country’s to step up too. The situation internationally is serious and warrants a concerted and serious response to defend the life of those with the extra love chromosome.
I think our work can easily be carried forward in Australia as their policies and laws pretty much mirror ours.
The situation in Europe is serious with high screening rates and termination rates (85% and 95% respectively in France, so around an 80% birth prevention rate of all pregnancies involving Down syndrome there). Mainland Europe is, however, well placed to take the Stop Eugenics Now initiative forward. The UK seems to have a problem with the silent roar of the crowd from the disability sector. The UK National Health Service is paying out compensation for wrongful birth claims and allowing babies with disabilities to be left to die, and we hear very little opposition from the disability sector – that is a concern, they need to find their voice.

In America, the International Down Syndrome Coalition is doing wonderful work around their message that all life is precious. The situation is serious there though; there is no legal protection against eugenic abortion. The national Down syndrome organisations seem to struggle with advocating for people with Down syndrome around prenatal screening. Look at the situation around providing information pamphlets for screening. Firstly NDSS, NDSC and GDSF published the Lettercase pamphlet, but included a reference to an option for abortion where there is a positive diagnosis. That’s not advocating for people with Down syndrome (hint, go back and read the bit about the new NZDSA position statements). Then NDSC and GDSF produce a new pamphlet, with no mention of abortion (great start), but then collaborate with testing company Sequenom to distribute the pamphlet (major fail). Collaborating with a company that markets a test to enable births of people with Down syndrome to be prevented is not advocating for people with Down syndrome.
It is good though that they are all talking about it and are aware of the risks of the new testing regime opening up there. The sort of life affirming positive messaging that the International Down Syndrome Coalition is doing can only do well there in the US.

On a local note, look out for the Christmas edition of Oh Baby magazine in New Zealand that comes out next week. It features our very work and gets our message out to our key audience – expectant mums and dads with wanted pregnancies. And that reflects how far we have come, people know about our work, they want to share our point of view and we are featured in mummy magazines. That’s fantastic.
Finally, I would like to thank all our wonderful supporters. We are very fortunate to have a number of international legal and medical experts supporting our work. People are stepping up to do research, prepare web sites, run facebook pages, organise and fund seminars and generally roll around in the thick of hard core advocacy.
People said we wouldn’t turn this around, but we said – we will do it anyway, because we can. Our families deserve nothing less of us. And turning this around, we are.
As we enter the period of Christmas I hope that you will celebrate this time in a way that is true for you and that there is a spirit of unconditional love in all that you do.
]]>
Last month Saving Downs held the “Loving Every Child: Defying Eugenics” seminar. Dr Deirdre Little gave an outstanding presentation on ‘Current practice and how it links with eugenics’. She gave a very detailed, scientific breakdown of what is really going on with routine antenatal screening programmes and their eugenic nature. It was timely, as there is a lot of smoke and mirrors going on around the place about screening and the new blood tests.
Take today’s article in the UK’s Telegraph for example, with the headline:
“Blood test for Down’s ‘could save 300 babies’ lives a year”
When you break it down, it actually means that saving of “normal” babies could be at the cost of over a further 700 babies with Down syndrome, resulting in a net increase in around 400 lives a year lost. The headline should read “Blood test for Down’s could cost 400 babies’ their lives per year”. I guess that doesn’t sound as good.
So, we have a misleading headline implying that the new blood test is a good thing as it saves lives, when the situation is the exact opposite. But then we have this:
“It therefore has the potential to all but eradicate Down’s syndrome”
Pardon me? Eradicate. Really? Well, yes that is the whole point, on this score they are being honest.
Let me share some of Dr Deirdre Little’s presentation that navigates through the fog. Her work is based on the Australian experience but equally applies hear in New Zealand and in the UK, as we have almost identical screening programmes. Most of what follows is credited to Dr Deirdre Little.
Each mother, at her first consultation for each pregnancy, is to be invited to consider the worth of her child. She is invited to submit her child for ‘consideration’ of whether he or she is worth having. No benefit is stated to Australian children from the new consideration.
That’s right. Mothers with wanted pregnancies are offered the opportunity to select their type of child based on a subjective assessment of another persons worth.
The National search for Down syndrome is now a population test. It should not be likened to other antenatal investigations and care, which aim to protect and further the health of mother and child. In days of Hippocratic principles of medicine, to the question: ‘how will this particular antenatal investigation help me or my child’ there was an answer. However, when that question is put to population testing for Down Syndrome: ‘how is it intended to help me or my child’ the answer is an offer to destroy the child within a legally timed framework.
There is no therapeutic justification for screening for Down syndrome during pregnancy – see our blog here. To be considered therapeutic in medical terms any proposed benefit has to outweigh the risk of procedural death to each child tested. Saving Downs has asked the New Zealand National Screening Unit for specific clinical evidence that there is a proportional therapeutic benefit to an unborn child and the mother that relies on a diagnosis of Down syndrome. They haven’t provided one piece of such evidence, despite investing $27M in their “quality improvement programme”.
The earliest amniocentesis foetal chromosome test for Down syndrome was in 1968. It was offered to older women who have a greater chance or “incidence” of Down syndrome births. Initially women over 40 years then women over 37 years were offered invasive testing. Openly eugenic, it declared in the “Australian Doctor” in March 2003:
“..where abortion laws permit, there is no need and no justification for delay in trying to institute a prenatal diagnostic screening programme for Down Syndrome. To effect the policy advocated here will bring relief to the community and new assurance to prospective parents”.
But medicine became dissatisfied. This method could only detect 70% of children with Down syndrome before birth. The other 30% occur in women under 37 years of age. Also raising concern, as was later referred to in the International Journal of Medical Sciences in 2005, this advanced maternal age group had included a disproportional number who would not accept termination for religious reasons and it included many (e.g. with infertility) who would not accept the hazards of invasive diagnosis.
So, as the decades passed, techniques of detection escalated to maximize live birth prevention of Down syndrome, to produce the curly and convoluted programme of screening and its targeting we have today.
In essence, the aim of prenatal testing is to maximize detection of Down syndrome for secondary prevention through selective abortion. The stated aim is to reduce the number of live Down syndrome births.
It has been estimated that $75,000 worth of screening goes into each Down Syndrome birth avoided. The MJA article looking at Down syndrome births in Queensland which had not reduced over a four year period of testing was disinterested in procedural mortality, concluding:
“recent economic analyses have shown that population based screening probably represents value for money. When the costs of screening are offset against the lifetime costs of caring for a person with Down syndrome, screening is less costly than no screening at all, regardless of which strategy is used.”
So we have a clear agenda here of birth prevention based on the might dollar.
A journal compilation published in ANZJOG in 2006, 46:92 -96 looking at population screening policy similarly concluded:
“For consideration of national policy, cost effective screening programmes will be significantly compromised if the participation rate is low… the costs of the screening programme to detect a certain number of cases has to be balanced against the cost of managing missed or undetected cases in the population… transport to and from (termination) facilities and ongoing grief counseling as well as the emotional cost of miscarriage.”
So we get to the truth of the matter. Screening programmes are significantly compromised if participation is low, or insufficient numbers of births are prevented. The UKs NHS even has an excel spreadsheet to evaluate screening programmes that require a termination rate to be entered by the evaluator along with the cost of stamps and phone calls. It would be funny if it wasn’t so dehumanising to our community.
No wonder parents feel they can’t outrun this. They have been left to outrun it on their own.
Dr Little concludes:
This test invades more than the womb and threatens more than the safety of the child, with neither proposal nor evidence of benefit, it invades the home, the family, the doctor-patient relationship and the security of society, which has a right to be protected from quasi- medical and tax-payer funded eugenic programmes.
Clearing the fog from prenatal genetic testing gives families back their autonomy and lets them breathe the free air again, as Tolkein would say. But not just free air, air lit with understanding, and enriched with guidance.
Dr Littles full presentation can be read here Current Practice and How it Links with Eugenics
]]>
There has been some interesting blogs going around objecting to Saving Downs using the term “eugenics” in relation to antenatal screening for Down syndrome. So, what’s really going here and how did we arrive at a government-funded eugenics programme in New Zealand in 2010?
Firstly, I should clarify that we use the term “screening” in the broad sense, applying to both screening to determine the chance of Down syndrome for the unborn child and diagnostic testing to confirm Down syndrome (albeit without complete certainty). When this technology is used for life affirming care for the unborn child and the parents, then that is antenatal health care and we support that.
When screening and diagnostic testing is used to select who gets born, based on the genetic difference of that child, then we have entered the realm of selecting the type of child, and it is eugenics. We oppose eugenics. It harms our community and it devalues the lives of those with Down syndrome.
So, what is eugenics? From Natalie Ball at Calgary University:
The term eugenics was coined by Sir Francis Galton in 1883 to refer to “the investigation under which men of a high type are produced”. Under Galton’s vision of eugenics, there are two ways that eugenics can be achieved: through increasing the frequency of so-called ‘desirable’ genes (known as positive eugenics), or decreasing the frequency of so-called ‘undesirable’ genes (known as negative eugenics). Eugenics is one dynamic that influences the judgment of people’s abilities and the disabling consequences.
Objections have been raised that eugenics has to involve some degree of enforcement by a government. This is incorrect. The French Council of State in its study on the revision of the bioethics laws in 2009 stated that:
“Eugenics may be the fruit of a policy deliberately carried out by a state. It may also be the collective result of a series of converging individual decisions taken by future parents in a society that seeks the production of the “perfect child” or the least one unaffected by numerous serious diseases”
Eugenics became popular in the early 20th century then quickly fell out of favour after the holocaust. It has now been resurrected under the guise of prenatal health care, reproductive choice, human rights and even “private decisions concerned with family’s well being”.
It is one of life’s great paradoxes that the most gentle, loving and enduring amongst us have always been the target of the eugenists – those with Down syndrome: the very people who embrace those defining human qualities of unconditional love and compassion so needed in this age. The Down syndrome community is first in line now, as it was in 1939 at the start of the holocaust. A case currently before the European Court of Human Rights even seeks to declare a fundamental human right to kill one’s unborn baby because it has Down syndrome through selective abortion. Unfortunately this is nothing new, and we do it now here in New Zealand.
It was back in the spring of 1939 that the infamous Action T4 programme was launched in Germany, the so-called euthanasia programme of the disabled. It had its origin in Binding’s and Hoche’s 1920 paper “Authorisation for the destruction of life unworthy of life”. The initial decree required midwives and physicians to report all infants born with disabilities to be reported to the T4 authorities. Number one on the list was “Mongolism”, that dated and offensive term of the time for people with a third 21st Chromosome: Trisomy 21 or Down syndrome. The first killings of the children started in October 1939 and quickly moved to adults. 70,000 disabled people were eventually killed as part of the holocaust that went on to include the gypsies and then the Jews. All in the name of racial hygiene and the eradication of those deemed to be unworthy of life. The Nazi Doctors involved where found guilty of crimes against humanity at Nuremberg and the practice of persecuting minority groups has been prohibited under international law ever since.
But the scourge of eugenics was to gain momentum in New Zealand in 1977 with the Royal Commission’s report on abortion, some 32 years after the holocaust. The Commission dealt with the issue of “handicapped” persons, stating:
“ It is not immoral to terminate a pregnancy where the fetus is likely to be born with a severe physical or mental handicap, because the burden of the handicapped person to himself and to his parents may be greater than the sum total of their happiness.”
Again, Down syndrome was the target of discussion, based in eugenic ideas that people with disabilities have “life unworthy of life” and their degree of burden exceeds their happiness. Of course any one with Down syndrome, or their families, will testify to the joy and love of their lives and the enrichment they bring to our society. New Zealand legalised the death of unborn children with disabilities in 1977, laying the grounds for eugenic abortion.
Under the radar the Ministry of Health has been running a screening programme for Down syndrome here since 1968 and the slippery slope was set in motion. In 2004 the National Screening Unit (NSU) began to review the programme, adding grease to the slope. They quietly noted enthusiastically that one of the purposes of their programme was to:
“allow couples at risk of anomaly to embark on having a family, knowing they may avoid the birth of seriously affected children through selective abortion”.
At the time the NSU were concerned that too many “normal” babies were being killed as a result of invasive tests and resulting miscarriages whilst trying to find the “defective” ones and that current practice had:
“failed to reduce the numbers of babies born with undiagnosed Trisomy 21”.
And so in 2010 the NSU brought in the “quality improved” programme to improve detection rates in spite of the basic facts that there is no therapeutic benefit in the programme and that participation in the screening pathway imposes more harm than benefit to an unborn child, through miscarriage and morbidity due to diagnostic testing.
The practice actually has more to do with money. It costs around $70,000 to detect an unborn child with Down syndrome and governments consider this to be cost-effective and cheaper than providing additional care, should it be required. The 2007 Health Outcomes report for the NSU says this about screening:
“It is cost-effective, as the estimated cost of avoiding the birth of a baby with Down syndrome is substantially less than the lifetime costs of care.”
Our children are reduced to a valueless disposable commodity.
Further grease was added to the slide with the introduction of new blood tests for Down syndrome in early pregnancy in America this year that are now being promoted in Europe, Australia and some Asian countries. People say this isn’t eugenics? Well what to the geneticists and bioethicists have to say then?
In March 2011 Philippos Patsalis of the Institute of Neurology and Genetics in Nicosia, who discovered the new technology, told reporters that:
“the cheaper and quicker method of blood sampling rather than collecting fluid from the womb will encourage more couples to take the test and therefore slowly eradicate the disease”
On 8 June 2012 Robert Klitzman, a bioethicist at Columbia University, made the following comment in relation to the use of these tests:
“This technology can enable us to eliminate some very serious diseases like Down syndrome”
So there we have it, no beating about the bush, it’s a disease and it needs to be eradicated through killing the person before birth. Classic eugenics worthy of Action T4 honours. Same intention: eradication, same outcome: eradication, same excuse: it’s a disease; these lives are unworthy of life.
But it doesn’t stop there though, now the de-selecting of the unborn with Down syndrome is being proclaimed as a human right. Forget the well-greased slippery slope of eugenic screening programmes and selective abortion; bring on the play ground slide for eradication as a right.
First there are a number of successful “wrongful birth” law suits in Europe and American where parents have successfully sued Doctors for not diagnosing their child with Down syndrome in the womb so that they could have killed them.
Then we had the two “bioethicists” in Australia argue that infanticide of children with Down syndrome should be permissive as:
“such children might be an unbearable burden on the family and on society as a whole”
Bioethicists? Yeah right – the new name for eugenicist.
And now we have a case before the European Court of Human Rights seeking to declare a fundamental human right to kill one’s unborn baby just because it has Down syndrome. Faced with the danger of prenatal screening and elimination becoming enshrined and consecrated as a human right the European Down syndrome community has launched an urgent mobilisation to petition the court. The petition appeals to the conscience of the Court and to European institutions to recognise the humanity, and protect the right to life, of people with Down syndrome and all disabilities. 38 European and International disability organisations have weighed in to support the petition.
Recognising as a human right the elimination of children with Down syndrome before their birth would stigmatise a human group selected on the basis of their genetic difference. A favourable ruling would simply deny the humanity of the persons with disabilities and setup in law the mechanism for their elimination through eugenics.
None of this makes for pleasant reading. Let us remember though that mothers who enter the screening pathway have wanted pregnancies. If there is an unexpected diagnosis then that is the first moment they are called to be true parents and provide unconditional love and support to their child. The inherent dignity and value of that wanted life is not suddenly eroded because there is a diagnosis of Down syndrome. As a civilised society we should be providing compassion and support in those situations and reaffirming our commitment to the same life affirming care that was there before the diagnosis. And we can be sure that the Down syndrome community will be there to support them.
]]>
There has been a bit of discussion going on around the place about screening for Down Syndrome having a therapeutic benefit. So what is the situation here in New Zealand?
Firstly, Saving Downs position is outlined in our Mission Statement:
To ensure that antenatal screening exists only to provide unborn children with Down Syndrome and their parents with life-affirming, unbiased care through education, support and understanding.
This is because we are advocates for people with Down Syndrome. Our view is that antenatal health care should be just that – supporting those wanted pregnancies through health care. We don’t recognise a role for screening to be used to prevent the births of children with the extra love chromosome, that is selection and eugenics.
Earlier this year Saving Downs made a submission to the National Screening Unit on the draft guidelines for health practitioners for antenatal screening for Down syndrome and other conditions. We made our position clear:
Saving Downs acknowledges that people with Down syndrome have an inalienable right to life from the moment of their conception until natural death, a right to be free from discrimination, and a right to be treated on an equal basis with all.
Saving Downs supports the use of screening only to promote safe birth outcomes for those who wish to have access to screening for this purpose.
Saving Downs opposes any form of antenatal screening and diagnostic testing that targets, and prevents, the birth of unborn children with Down syndrome, or causes harm to any unborn child.
So, where does therapeutic benefit fit in to all of this? From our submission:
In medical considerations, a proposed theoretical scenario of benefit or ‘beneficence’ would need to be statistically more likely to provide therapeutic gain than the stipulated Royal Australian and New Zealand College of Obstetricians and Gynecologists (RANZCOG) foetal mortality rate. The benefit or gain it proposes would also need to be proportional to the significance of the hazard imposed on the tested individual, i.e. death. If these criteria are not fulfilled, then the test is non-therapeutic.
Invasive prenatal diagnosis carries a RANZCOG stipulated additional foetal mortality rate of up to 3% for CVS and up to 1% for amniocentesis (both in addition to the normal miscarriage rate), and with increased foetal mortality rates in trainee hands. This risk to the foetus is considered disproportional to the comfort of foreknowledge, and disproportional to the known facts that conditions whose managed survival outcome is deemed dependent on invasive testing are rarer than the testing death rate.
The difference between therapeutic and non-therapeutic testing is an important explanation to give to parents. We submit that pregnant women and their partners must be advised that the screening pathway is non-therapeutic and that must be made very clear in the outset for facilitating informed consent.
We submit that pregnant women and their partners must be advised that participation in the screening pathway imposes more harm than benefit to their unborn child, through miscarriage and morbidity due to diagnostic testing.
That’s all a bit technical. It simple terms it means that if one enters the diagnostic (invasive test) part of the screening pathway, then on balance the unborn child will exposed to more harm than good. So, we believe that parents who want the information to be prepared need to understand this risk before they enter the screening pathway.
There are other risks to, miscarriage rates have been assessed as being 6 to 8 times higher than average in trainee hands. And what about other harm to the unborn child other than miscarriage from the diagnostic test, that we never hear about? Again, from our submission:
Apart from foetal testing mortality rates there are foetal morbidity rates which the mother needs to consider before consenting to the screening pathway. Limb deformities, lung problems, infection and other consequences of slow ongoing amniotic fluid leaks have been well documented. This morbidity and other complications are not mentioned anywhere in the draft health practitioners document.
We submit that pregnant women and their partners must be advised of the mortality and morbidity rates associated with each test and the additional risks associated with trainee practitioners.
Wrapping all that up in our submission to the National Screening Unit we said:
The difference between therapeutic testing and non-therapeutic testing is one which will need to be made very clear in the outset, again for reasons of informed consent.
Screening cannot itself diagnose or identify. It can only point one in twenty mothers, those 5% of the whole New Zealand population who will screen at increased risk, to invasively test or not. Invasive prenatal diagnosis carries a RANZCOG stipulated additional foetal mortality rate of up to 3% for CVS and up to 1% for amniocentesis (both in addition to the normal miscarriage rate) with increased foetal mortality rates in trainee hands. This risk to the foetus will be considered disproportional to the comfort of foreknowledge, and disproportional to the known facts that conditions whose managed survival outcome is deemed dependent on invasive testing are rarer than the testing death rate.
Any scenario postulated of benefit, to be genuine, should be investigated with an invasive test done as late as feasible in the pregnancy, to avoid foetal death, and risk only foetal prematurity.
The difference between therapeutic and non-therapeutic testing is an important explanation to give to parents.
We submit that all misleading assertions overstating what screening can actually achieve be corrected.
We submit that pregnant women and their partners must be advised that the screening pathway is non-therapeutic and that must be made very clear in the outset for facilitating informed consent.
To summarise then, there are real risks associated with the invasive testing stage of the screening pathway. We understand that some parents want this information and we want them to be fully aware of these risks before making that decision.
As an advocacy group for people with Down Syndrome we only support screening for life affirming care and support parents who want to use it for that purpose. However, parents should be aware of the potential harm to their children if they enter the invasive testing stage. In medical terms the level of harm across the population exceeds any medical benefit that relies on a diagnosis of Down Syndrome. Essentially it is a programme to screen Down Syndrome out of the New Zealand population.
]]>The previously mandated offering of screening sent an implicit message to mothers that participation in the screening programme was the “right” thing to do. As the programme has a stated objective and outcome of preventing the birth of children with Down syndrome and other disabilities, the mandated offering of screening offends principles of human dignity and diversity. Such programmes are recognised as eugenic.
SavingDowns spokesman Mike Sullivan says that feedback from midwives and GPs attending the current NSU training workshops on screening for Down syndrome and other conditions indicates a growing opposition to the screening programme, on the grounds that the eugenic undertone is unethical. “We concur with the new position statement from the New Zealand Down Syndrome Association that it does not consider Down syndrome in itself a reason for termination (of a pregnancy)”, he said.
By changing the requirement for midwives and GPs from “offering” screening to simply “advising” pregnant women of its availability, the onus is on the parents to request participation, rather than it being a matter of routine pregnancy care. Midwives and GPs who are morally opposed to eugenics can exercise their right to conscientious objection and advise parents to seek the “service” elsewhere with no requirement to provide a referral (as provided for under Section 174 of the Health Practitioners Competence Assurance Act 2003). They are also free to explain that the screening pathway has no therapeutic benefit for their child.
Mr Sullivan described the new policy as “a step in the right direction for respecting the lives of those with Down syndrome and other disabilities”.
In 2010, a complaint from SavingDowns was upheld by the Health and Disability Commissioner on the unbalanced quality of information produced by the NSU. As a result of this the NSU has been revising its guidelines for health practitioners. The refocus away from the routine offering of screening is a direct result of submissions received by the NSU on the draft revised guidelines from the disability community. The NSU is also revising their consumer resources, as the current series of three pamphlets given to pregnant women were also deemed inadequate by the Health and Disability Commissioner.
Mr Sullivan notes that “when a pregnant woman sees her midwife or GP, she has a wanted pregnancy and is seeking nurturance through to a successful birth”. SavingDowns calls on health professionals to act with conscience and dignity and do their utmost to respect all human life, including those with Down syndrome and other disabilities.
ENDS
For more information contact:
Mike Sullivan
Spokesman for SavingDowns
09 436 1498
021 406 266
[email protected]